COVID-19 Is Expected to Have Long-term Impact on Oncology Practices
The rapidly developing nature of our knowledge about the coronavirus disease 2019 and the need to respond quickly to the pandemic are prompting community oncologists to search for ways to maintain their practices while improving the quality of care for their patients.

The rapidly developing nature of our knowledge about the coronavirus disease 2019 (COVID-19) and the need to respond quickly to the pandemic are prompting community oncologists to search for ways to maintain their practices while improving the quality of care for their patients.
Oncology practices are spending more on resources while not seeing the volume of patients they once did. Early data indicate that the crisis is having a significant financial impact on community oncology practices, which have reported steep decreases in patient visits, treatments, and new patients.
“We are just beginning to see the tip of the iceberg of the impact on practices and what the financial impact will be,” Jeff Vacirca, MD, chief executive officer of New York Cancer and Blood Specialists (NYCBS), said in an interview with OncologyLive®. “COVID-19 is going to leave a lot of smaller community cancer practices in financial trouble. Oncology practices depend on referrals and referrals depend on surgeries. We have seen elective surgeries now shut down for well over 6 weeks. We’re going to continue to see this impact through the next quarter.”
Medical groups of all sizes and specialties have felt the direct and indirect financial impact of the COVID-19 pandemic, according to a survey of practices that the Medical Group Management Association conducted on April 7 and 8, 2020.1 Although not specific to the oncology field, the survey found on average that practices reported a 55% decrease in revenue and a 60% decrease in patient volume since the beginning of the COVID-19 pandemic. Thirty-six percent of respondents projected there would be layoffs at their practices by May 8 and 60% expected furloughs.1
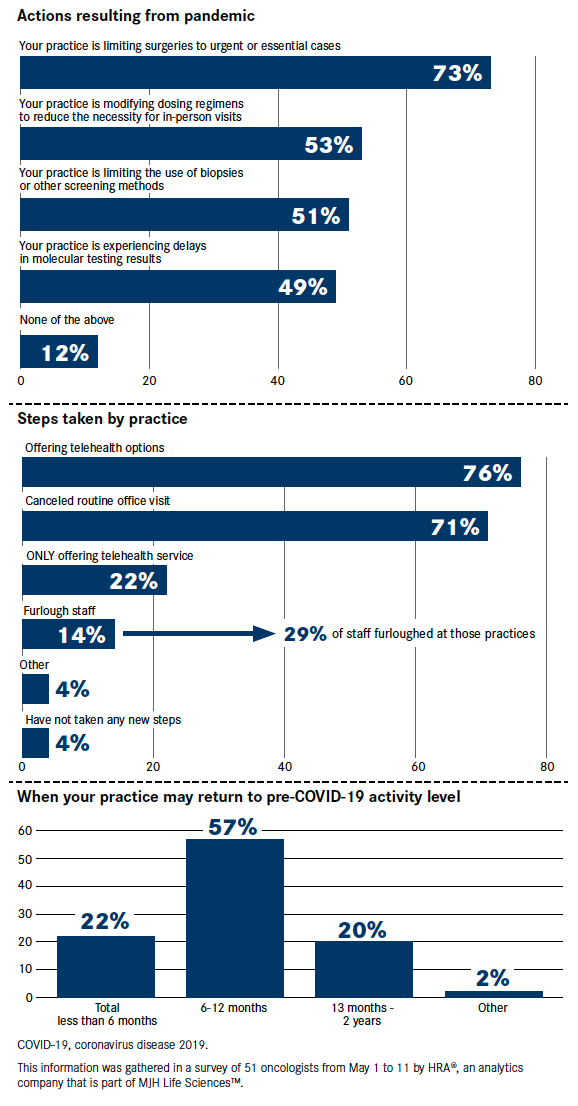
The impact of the pandemic on oncology practice specifically is widespread, according to a report from HRA®, an analytics company that is part of the MJH Life Sciences™ family of health care services, which includes OncLive®. In an in-depth survey of 51 US oncologists conducted from May 1 to May 11, 73% said they were limiting surgeries to urgent or essential cases and 53% had modified dosing regimens to reduce the need for in-person visits. Additionally, 71% had canceled routine office visits and 14% had cut staff. Among those practices that did make staffing cuts, they furloughed 29% of the staff. On a positive note, 57% of the respondents said they expected their practice to return to pre–COVID-19 levels within 6 to 12 months (Figure).
There is a concern that practices that were hanging on are going to be in a tight space, Ted Okon, executive director of the Community Oncology Alliance (COA), said in an interview. “We’re going to see some clinics closing. We’ll see some clinics bought by hospitals. There are some hospitals that are so well endowed…they will have a lot of resources to be able to grab up cancer practices.”
Vacirca says he hopes there is a reset for the cancer care community and hospital systems. “Hospitals systems have learned that they need to be ready for a health care crisis like this and perhaps not concentrate all their time and effort to acquiring practices just for the sake of profit taking.”
Federal Programs Offer Funding
In the meantime, practices have been able to take advantage of some federal relief efforts, such as the Paycheck Protection Program or grants from the Department of Health and Human Services (HHS).
Starting in April, the Coronavirus Aid, Relief, and Economic Security Act provided $100 billion to support providers’ health care–related expenses or lost revenue attributable to COVID-19 and to help cover testing and treatment for uninsured Americans. A portion of that funding, $50 billion, was offered as grants to hospitals and providers based on their net patient revenue for 2018.2,3 Grants were given in 2 waves, according to a spokesman for HHS. The first wave of $30 billion was based on Medicare fee-for-service reimbursements for 2019. The second wave of $20 billion was calculated so that both grants in total were proportional to providers’ share of 2018 revenue.
Additionally, the Centers for Medicare & Medicaid Services (CMS) in April delivered nearly $34 billion to health care providers through the expansion of the Accelerated and Advance Payment Program.4 The payments are available to providers who participate in the Hospital Insurance (Part A) and Supplementary Medical Insurance (Part B) programs. The advance payments are separate from the HHS grants and are considered a loan that providers must pay back.
Practice Details Provide a Snapshot
One oncology practice, NYCBS, a multispecialty practice with more than 25 sites across Long Island and New York City, felt the significant impact on care delivery and practice operations due to COVID-19. By the end of March, its weekly average cancellation rate increased by 80%.
NYCBS moved quickly to implement remote visits using telehealth for patients as the pandemic escalated in the greater New York City area. The practice worked with the revenue cycle management team at Flatiron Health to define and track new key performance indicators to report on how remote services were being adopted. Initial results from these efforts indicated a 51.2% acceptance rate for remote visits.
“The moment [CMS] gave the go-ahead for remote visits, the Flatiron team along with my team here at NY Cancer had that system up and running within 24 hours,” Vacirca said. “Patients are so grateful that we were able to keep their care continuous throughout this pandemic.
“I believe that remote visits are going to be how we conduct cancer care moving forward,” he added. “It’s not just important for those patients who have a hard time traveling; it’s also important for patients who need second opinions and it’s important for patients who are sick and at home. It makes a huge difference in patient care.”
The team at NYCBS also recognized a need to change their approach to reach even more patients. The practice implemented drivethrough services for laboratory and injection services. Additionally, they created a waiting room workflow for in-person appointments that enables patients to check in remotely and wait outside of the clinic until their provider is ready.
After implementing these additional options, the practice saw adoption rates of 70% for drive-through services and 77% for remote waiting rooms. Meanwhile, NYCBS’ cancellation rate decreased and stabilized close to the 2020 weekly average prior to COVID-19.
Although Vacirca said these were important steps to take during the pandemic to ensure patients received care, he would like to get patients back into the office. “Operationally, it works better when people are in the office but at least we know if there is a situation like this again in the future and until this situation ends, we are able to provide the level of care we always have.”
Practice Mergers are Expected to Continue
Although government support and policy changes are helping practices weather the storm, it is unclear if such measures will be enough to stave off consolidation and closures in the future. “It’s perhaps likely, that the painful process of reaching a new health care equilibrium will last well into 2021,” Cutler et al wrote in a recent commentary in JAMA.5
Cancer care providers continue to grapple with financial pressures, according to the 2020 Community Oncology Alliance Practice Impact Report. Since 2018, 99 practices have been acquired by hospitals, or have merged with or have been acquired by another community oncology practice or corporate entity, representing a 12% increase.6 This report was researched before the COVID-19 pandemic, and Okon expects the trend of mergers and acquisitions to continue as community practices deal with the outbreak’s ramifications.
Compiled from public and private data sources, the report provides a look at community oncology trends at the national and state levels over a 12-year period, from January 2008 through April 2020. Since 2008, COA has tracked 435 community oncology practices that have closed, 722 that have been acquired or have become affiliated with hospitals, and 203 that have been merged or acquired by other entities.
The hospital acquisitions, which increased 9.7% from 2008 to 2020, are fueled mostly by financial incentives in the 340B Drug Discount Program and higher payments for cancer care services performed at hospitals, according to COA.6 Under the 340B program, eligible hospitals are able to obtain drugs at discounted prices and bill private insurers and Medicare at higher rates. Community oncology providers say they cannot compete with the higher margins available to hospitals under the program.7
Okon says COA’s report shows that policymakers in Washington are still not doing enough to preserve the independent community oncology system. “At the same time, we are being driven by public policy to deliver higher value and lower costs, all while not enough is being done to stop cancer care from being shifted into the much more expensive hospital setting,” he said in a press release. “The shifting of cancer care to large health systems is the result of the runaway 340B program and disparate site-of-service payments that basically mint money for hospitals.”
New Ways of Working are Benefiting Patients
Cancer care post-COVID-19 will likely look very different from what it did before the pandemic. In fact, social distancing, electronic communications, the implementation of telehealth, and other changes that practices made to their operations to keep their patients and staff safe during this pandemic are likely here to stay.
Five years from now, interactions with patients will be more frequent, use electronic communications, and will try to connect the various pieces of a patient’s journey, Barry Russo, MBA, chief executive officer, The Center for Cancer and Blood Disorders in Fort Worth, Texas, said at the 2020 COA Annual Conference, held virtually on April 23 and April 24.
“What we are learning in value-based care is that everything going on with the patients―with their rheumatologist, their pulmonologist, their cardiologist, their psychiatrist, their podiatrist even―are part of the journey,” he said. “In many cases, we have not had good insight into that.”
Connections with other providers will make a difference in how clinicians take care of patients, Robert P. Braun, vice president of operations and integration, Regional Cancer Care Associates in Hackensack, New Jersey, said at the meeting. “It will force us to change how we work with other providers. There are so many things going on with a patient and, because of the electronic world, we’re going to have a better picture of the patients and that will impact how we will care for them.”
Some speakers at the COA meeting suggested nonclinical staff working remotely could continue after the pandemic ends. “There may be portions that can stay remote,” said Steve D’Amato, BScPharm, executive director and clinical pharmacy specialist New England Cancer Specialists in Scarborough, Maine. “That will become important as we look at space going forward. The remote location of staff may have created some redundancies and some opportunities.”
Recognizing the strain that COVID-19 has had on the cancer care system, the American Society of Clinical Oncology launched in late April a “Road to Recovery” initiative.8 This project will examine how the COVID-19 crisis has affected the oncology field and what a new “normal” could look like. The society will convene 2 multidisciplinary working groups that will evaluate how changes in care delivery and clinical research could serve as lessons for new approaches that could improve care or help support recovery efforts in the future. An action plan with recommendations for policy or practices needed to support recovery is expected by September 2020.
References
1. COVID-19 financial impact on medical practices. Medical Group Management Association. Accessed April 28, 2020. https://mgma.com/getattachment/9b8be0c2-0744-41bf-864f-04007d6adbd2/2004-G09621D-COVID-Financial-Impact-One-Pager-8-5×11-MW-2.pdf.aspx?lang=en-US&ext=.pdf
2. US Department of Health and Human Services. HHS to begin immediate delivery of initial $30 billion of CARES Act provider relief funding. Published April 10. Accessed May 11, 2020. bit.ly/2Lqxoy0
3. HHS announces additional allocations of CARES Act provider relief fund. US Department of Health and Human Services. Published April 22, 2020. Accessed May 11, 2020. bit.ly/2LopRjt
4. CMS approves approximately $34 billion for providers with the accelerated/advance payment program for Medicare providers in one week. Centers for Medicare & Medicaid Services. Published April 7, 2020. Accessed May 11, 2020. https://www.cms.gov/newsroom/press-releases/cms-approves-approximately-34-billion-providers-acceleratedadvance-payment-program-medicare
5. Cutler D, Nikpay S, Huckman RS. The business of medicine in the era of COVID-19. JAMA. Published online May 1, 2020. doi:10.1001/jama.2020.7242
6. Community Oncology Alliance. 2020 Practice Impact Report. April 24, 2020. Accessed April 28, 2020. bit.ly/3bXZmwA
7. McCaughan M. Health policy brief: the 340B drug discount program. Health Aff. Published September 14, 2017. Accessed April 28, 2020. doi:10.1377/hpb20171024.663441
8. American Society of Clinical Oncology. The road to recovery: cancer care and research in a post-COVID-19 world. Published April 23, 2020. Accessed May 8, 2020. bit.ly/3dLxX1H
Source:OncLive By: Denise Myshko
Support families fighting financial toxicity of cancer – here